Identify the type of wounds in the pictures below.

Wounds may be acute or chronic and classified as partial or full-thickness.
Common types of wounds
We will review five common types of wounds; pressure wounds, venous ulcers, arterial ulcers, diabetic foot ulcer or neuropathic ulcers, and skin tears. Here are their descriptions:
Pressure injury is localized damage to the skin and/or underlying soft tissue, usually occurring over bony prominences and typically have a circular appearance.
Venous ulcers, also referred to as stasis ulcers, insufficiency or varicose ulcers, are the result of malfunctioning venous valves causing pressure in the veins to increase. Three theories have been advanced to describe the pathogenesis of venous ulcers (Agale SV. 2013).
Venous Ulcer Pathogenesis (theories)
- "Fibrin cuff" theory
- venous hypertension causes capillary dilation which leads to extravasation (leakage) of fibrinogens into the interstitium. Fibrin deposited around the capillaries form a "cuff" that decreases permeability to oxygen and nutrients, leading to tissue hypoxia, necrosis and poor wound healing.
- Inflammatory trap theory
- venous hypertension slows capillary blood flow which increases leukocyte adhesion to capillary endothelium. Adhesion of leukocytes to capillary endothelium activates the release of inflammatory mediators and reactive oxygen species that destroy capillaries resulting in localized ischemia.
- Microangiopathy theory
- intracapillary stasis promotes microthrombi that reduce nutrition and oxygenation predisposing to ulceration.
Venous ulcers are usually found on the medial or lateral distal (lower) leg. Venous ulcers generally have irregularly shaped edges and may have dark discoloration of the surrounding skin.
Arterial ulcers are full-thickness skin breakdown due to ischemia resulting from arterial insufficiency (Dendale, 2106).
Arterial ulcer pathogenesis
- Arterial insufficiency can slow healing.
- Slow healing increases the risk of a minor injury becoming an arterial ulcer.
- Ischemia resulting from severe arterial disease can cause spontaneous localized necrosis and slow healing.
Characteristics of arterial ulcers may include
- Usually located on the lower legs and the feet, and may be acute, recurrent or chronic.
- Arterial Ulcers are generally painful, particularly at night.
- They are uniform in shape with well-defined borders.
- Cool, pale or bluish skin that appears shiny and little of no leg hair.(Dendale, 2016)
- Faint or absent ankle pulses.
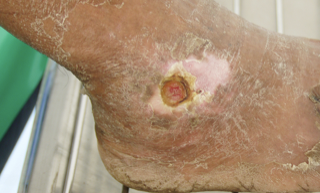
Diabetic foot ulcers or neuropathic ulcer result from parathesias or decreased sensation over pressure points that cause extended microtrauma. This type of ulcer may have a “ punched out” appearance ( Cox, 2019, WoundSource nd)
Skin tears look like cutes they are typically painful and tend to bleed. Most often found on hands and arms. Sometimes they occur on lower leg. Generally, they are found where the skin is thin. Common in elderly patient where the skin is fragile and has lost a lot of elasticity
Instant feedback:
Identify the type of wounds in the pictures below.



References
Agale SV. (2013) Chronic Leg Ulcers: Epidemiology, Aetiopathogenesis, and Management. Hindawi. Vol. 2013, 413604.
Cox, J. (2019). Wound Care 101, Nursing 2019. 49(10), 32 – 39.
Dendale, A. (2016). Arterial Ulcers. DermNet NZ retrieved from https://dermnetnz.org/topics/arterial-ulcer/
Wound Source (nd) Venous Insufficiency Ulcers retrieved from https://www.woundsource.com/print/patientcondition/venous-insufficiency-ulcers
Wound source (nd) Diabetic Foot Ulcers: Neuropathic https://www.woundsource.com/patientcondition/diabetic-foot-ulcers-neuropathic
© RnCeus.com