Arterial Blood Pressure Monitoring
Peripheral intra-arterial catheters ("arterial lines, a-line") offer clinicians a reliable method for continuous and direct monitoring of intra-arterial pressure (IAP). IAP monitoring begins when the left ventricular systole ejects blood from the heart into the aorta creating a fluid pressure wave. The fluid pressure wave is transmitted from the aorta to the peripheral arterial vasculature. For convenience and safety the arterial pressure wave is usually monitored at the radial, brachial, femoral and dorsalis pedis arteries. (Click for common palpation points)
Indications for IAP monitoring
- When the need for continuous beat-to-beat blood pressure is anticipated: e.g., significant blood loss, major surgery, comorbidities, etc.
- Titration of vasopressor or anti-hypertensive medications for the management of critically ill hemodynamically unstable patients
- Frequent sampling of blood, e.g. sequential blood gas draws, multiple hemoglobin and hematocrit
- Arterial administration of drugs, e.g. thrombolytics
- Insertion of intra-aortic balloon pump (femoral artery)
- Real-time calculation of cardiac output, stroke volume, and evaluation of fluid responsiveness
- When a hemodynamically unstable patients cannot be monitored with non-invasive methods, e.g. "large surface area burns, severe hypotension, multiple extremity fractures, or extreme obesity" (Hager 2021).
Contraindications for IAP catheter insertion
- Insufficient collateral circulation
- Skin defect over planned insertion site
- Synthetic vascular graph
- Raynaud syndrome
- Cautionary conditions:
- anticoagulation, e.g. thrombolytics for an acute infarct
- coagulopathy
- atherosclerosis
- etc.
Complications
- Bloodstream infection (BSI)
- O'Horo, Maki, Krupp, Safdar (2014) meta-analysis of 49 studies found
- Arterial catheters are a significant source of BSI (3.4/1000 catheters)
- Radial artery catheter infection rate was lower than femoral catheter.
- Rickard, Marsh, Larsen, McGrail, et al. (2021) compared CVAD and peripheral arterial line (PAL) rate of BSI in adults and children (n=6007) when infusion sets were replaced at 7-day or 4-day intervals.
- The CVAD-BSI rate was 1.78% of 7-day group and 1.46% of the 4-day group
- The PAL-BSI rate was 0.28% of 7-day group and 0.0% 4-day group.
- Singh, Bahadorani, Wakefield, Makarov, et al. (2017) found that among 21,597 cardiac surgery patients monitored by brachial artery cannulation (BAC),
- 0.19% had a vascular, nerve or local infection injury as a consequence of BAC
- 0.15% BAC associated injuries were vascular
- 0.04% of BAC associated injuries were from infection
- peripheral artery disease was associated with increased risk of BAC complications
- BAC complications were associated with prolonged hospitalization and in-hospital mortality.
- Radial artery spasm is treated with intra-arterial verapamil and/or nitroglycerine (Riangwiwat 2021)
- Hemorrhagic complications include perforation, hematoma, arteriovenous fistula, and pseudoaneurysm, all are treated with prolonged compression (Riangwiwat 2021)
- Radial artery occlusion prevention includes Barbeau test and appropriate anticoagulation (Riangwiwat 2021).
Common insertion sites
Radial artery
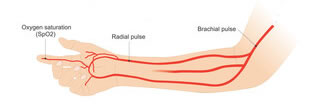 The brachial artery divides at the cubital fossa to form the radial and ulnar arteries. The radial artery is commonly used for arterial line placement because it is readily accessible and has a low complication rate (Nutall 2016). "It is palpable at the wrist, proximal to the radial styloid or radial head and slightly lateral. The cannulation site should be at the very distal portion of the arm. The most frequent location for radial artery cannulation is at the proximal flexor crease of the wrist, 1 cm proximal to the styloid process" (Hager 2021). The radial and ulnar arteries supply the deep and superficial palmar arches which provide collateral circulation.
The brachial artery divides at the cubital fossa to form the radial and ulnar arteries. The radial artery is commonly used for arterial line placement because it is readily accessible and has a low complication rate (Nutall 2016). "It is palpable at the wrist, proximal to the radial styloid or radial head and slightly lateral. The cannulation site should be at the very distal portion of the arm. The most frequent location for radial artery cannulation is at the proximal flexor crease of the wrist, 1 cm proximal to the styloid process" (Hager 2021). The radial and ulnar arteries supply the deep and superficial palmar arches which provide collateral circulation.
Femoral artery
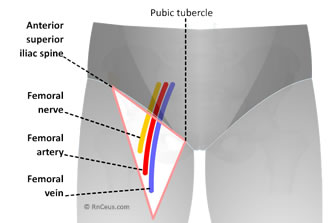 The femoral artery is a large caliber vessel that may facilitate emergent access for severely hypotensive or coding patients. It provides pressure measurements that are less affected by peripheral vasoconstriction, but significant leakage of blood into the surrounding tissue can occur without detection.
The femoral artery is a large caliber vessel that may facilitate emergent access for severely hypotensive or coding patients. It provides pressure measurements that are less affected by peripheral vasoconstriction, but significant leakage of blood into the surrounding tissue can occur without detection.
The femoral artery cannulation site is located at the groin, in the inner thigh, at the mid-inguinal point, halfway between the pubic symphysis and anterior superior iliac spine.
Cannula insertion risk reduction
Identify contraindications and avoid complications, begin with a checklist
- Valid insertion order
- 2 forms of patient ID.
- Informed consent,
- Review patient history,
- Verify appropriate equipment,
- Verify approriately trained personnel,
- Initiate physical assessment,
Skin changes, scars, sores, discoloration, swelling, excess warmth or swelling etc., could indicate the presence of peripheral vascular disease.
Palpation, capillary refill and the Allen test  are necessary steps to determine the suitability of a limb for insertion of an arterial line. The Allen test determines the patency of the arm's radial and ulnar arteries. The Allen test must be done prior to arterial line insertion, in order to reduce the risk of ischemia due to arterial occlusion.
are necessary steps to determine the suitability of a limb for insertion of an arterial line. The Allen test determines the patency of the arm's radial and ulnar arteries. The Allen test must be done prior to arterial line insertion, in order to reduce the risk of ischemia due to arterial occlusion.
- Ask patient to place hand, palm up, on the knee.
- Using both of your thumbs, compress the radial and ulnar arteries.
- Ask patient to open and close a fist several times, watch for blanching of the palm.
- Release only the radial artery; palm should become pink in seconds.
- Repeat process this time releasing only the ulnar artery.
- If the palm remains blanched when either the radial or ulnar arteries are released, there may not be sufficient circulation if a catheter were to be inserted.
| CDC Recommendation Peripheral Arterial Catheters and Pressure Monitoring Devices for Adult and Pediatric Patients |
| 1. |
In adults, use of the radial, brachial or dorsalis pedis sites is preferred over the femoral or axillary sites of insertion to reduce the risk of infection.
In adults, use of the radial, brachial or dorsalis pedis sites is preferred over the femoral or axillary sites of insertion to reduce the risk of infection |
| 2. |
In children, the brachial site should not be used. The radial, dorsalis pedis, and posterior tibial sites are preferred over the femoral or axillary sites of insertion. |
| 3. |
A minimum of a cap, mask, sterile gloves and a small sterile fenestrated drape should be used during peripheral arterial catheter insertion. |
| 4. |
During axillary or femoral artery catheter insertion, maximal sterile barriers precautions should be used. |
| 5. |
Replace arterial catheters only when there is a clinical indication. |
| 6. |
Remove the arterial catheter as soon as it is no longer needed. |
| 7. |
Use disposable, rather than reusable, transducer assemblies when possible. |
| 8. |
Do not routinely replace arterial catheters to prevent catheter-related infections. |
| 9. |
Replace disposable or reusable transducers at 96-hour intervals. Replace other components of the system (including the tubing, continuous-flush device, and flush solution) at the time the transducer is replaced. |
| 10. |
Keep all components of the pressure monitoring system (including calibration devices and flush solution) sterile. |
| 11. |
Minimize the number of manipulations of and entries into the pressure monitoring system. Use a closed flush system (i.e., continuous flush), rather than an open system (i.e., one that requires a syringe and stopcock), to maintain the patency of the pressure monitoring catheters. |
| 12. |
When the pressure monitoring system is accessed through a diaphragm, rather than a stopcock, scrub the diaphragm with an appropriate antiseptic before accessing the system. |
| 13. |
Do not administer dextrose-containing solutions or parenteral nutrition fluids through the pressure monitoring circuit. |
| 14. |
Sterilize reusable transducers according to the manufacturers’ instructions if the use of disposable transducers is not feasible. |
Centers for Disease Control and Prevention. (2015, November 5). BSI. Centers for Disease Control and Prevention. Retrieved December 27, 2021, from https://www.cdc.gov/infectioncontrol/guidelines/bsi/index.html#rec17
|
Set-up checklist:
Sterile barrier precautions (surgical mask, sterile gloves, cap, sterile gown, and sterile drape)
Skin cleaning with alcohol-based chlorhexidine(rather than iodine)
Specified staff for line insertion, i.e. competency training/assessment
Standardized insertion packs
Checklist completion by trained observer
Prepare ultrasound guidance for insertion
Verify that the pressure tubing/transducer assembly is:
properly connected to the monitoring equipment
connected to 500ml saline in IV fluids cuff with gauge & pump set to 300mmHg
properly flushed of all air and functioning, i.e. square wave when flushed.
Aseptic Insertion by approved personnel
- Adhere to the institution's arterial catheter insertion bundle (ACIB)
- Catheter is inserted in compliance with manufacturer requirements (30-degree angle)
- Aseptic technique to connect catheter hub to the non-flexible tubing/transducer assembly and properly flush
- Confirm proper arterial waveform, reposition as needed
- Cleans area, secure and apply dressing per ACIB,
- Positioned transducer level with the heart, then "zero" to negate the pressure applied by the saline or heparinized flush
- When zeroed, the transducer will reflect changes in the intra-arterial pressure.
Waveform evaluation is the best method to determine correct placement.
The normal peripheral arterial waveform will display the peak systolic pressure after the QRS. This phenomenon reflects the time it takes the cardiac systolic pressure wave to reach the peripheral catheter and sensor. The dicrotic notch reflects the closure of the aortic valve. Of course, the aortic valve has closed prior to the display of the notch.
The time delay is a function of both distance and compliance and elasticity of the vessels. The waveform of a patient with arteriosclerotic disease would be steeper in ascent and descent, therefore shorter in duration and the notch would be less well defined.
Correlation of pressure readings with contralateral blood pressure cuff should be done periodically, if possible.
Instant Feedback:
The normal arterial waveform will display a "dicrotic" notch, reflecting the closure of the aortic valve.
References
Hager HH, Burns B. ( 2021) Artery Cannulation. [Updated 2021 Jul 31]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; Available from: https://www.ncbi.nlm.nih.gov/books/NBK482242/
Nuttall G., Burckhardt J., Hadley A., Kane S., Kor D., Shirk Marienau M. , Schroeder D.R., Handlogten K., Wilson G., Oliver W.C. (2016) Surgical and Patient Risk Factors for Severe Arterial Line Complications in Adults. Anesthesiology; 124:590–597 doi: https://doi.org/10.1097/ALN.0000000000000967
O'Horo JC, Maki DG, Krupp AE, Safdar N. Arterial catheters as a source of bloodstream infection: a systematic review and meta-analysis. Crit Care Med. 2014 Jun;42(6):1334-9. doi: 10.1097/CCM.0000000000000166. PMID: 24413576.
Riangwiwat T, Blankenship J.C. (2021). Vascular Complications of Transradial Access for Cardiac Catheterization. US Cardiology Review 2021;15:e04. DOI:https://doi.org/10.15420/usc.2020.23
Rickard, C. M., Marsh, N. M., Larsen, E. N., McGrail, M. R., Graves, N., Runnegar, N., Webster, J., Corley, A., McMillan, D., Gowardman, J. R., Long, D. A., Fraser, J. F., Gill, F. J., Young, J., Murgo, M., Alexandrou, E., Choudhury, M. A., Chan, R. J., Gavin, N. C., … Playford, E. G. (2021). Effect of infusion set replacement intervals on catheter-related bloodstream infections (RSVP): A randomised, controlled, equivalence (central venous access device)–non-inferiority (peripheral arterial catheter) trial. The Lancet, 397(10283), 1447–1458. https://doi.org/10.1016/s0140-6736(21)00351-2
© RnCeus.com