Coanalgesic Drugs
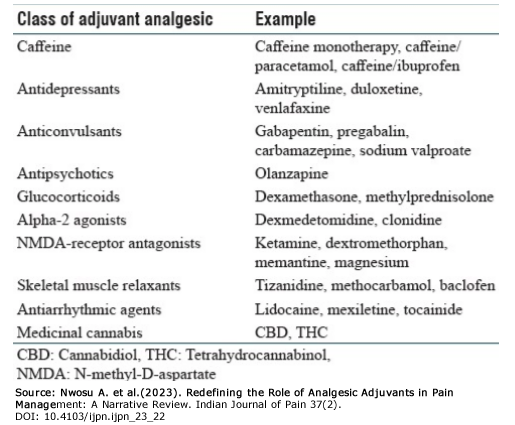 Coanalgesics, or adjuvant drugs, are medications whose primary indication is for a purpose other than pain relief but that demonstrate some analgesic effects (Portenoy R. K. 2020). Antidepressants, anticonvulsants, corticosteroids, and other drugs may be used as coanalgesics. Coanalgesics may be used in addition to other analgesics or alone as primary treatment for specific painful conditions. Most experience with coanalgesics has been in treating chronic pain, but adjuvant analgesics are increasingly being used to treat acute pain (Imani, F., & Varrassi, G. 2019). (Click table to expand, and again to minimize)
Coanalgesics, or adjuvant drugs, are medications whose primary indication is for a purpose other than pain relief but that demonstrate some analgesic effects (Portenoy R. K. 2020). Antidepressants, anticonvulsants, corticosteroids, and other drugs may be used as coanalgesics. Coanalgesics may be used in addition to other analgesics or alone as primary treatment for specific painful conditions. Most experience with coanalgesics has been in treating chronic pain, but adjuvant analgesics are increasingly being used to treat acute pain (Imani, F., & Varrassi, G. 2019). (Click table to expand, and again to minimize)
An opioid analgesic should be introduced and titrated to a maximum effect before a coanalgesic is added to the pain management regimen. The reason for this is that when both drugs are introduced together, the risk of toxicity increases. Increases. It may be difficult to determine which drug is responsible for producing analgesia or causing side effects. Fewer patients experience pain relief from coanalgesics alone than from opioid analgesics.
Most co-analgesics have a slower onset of analgesic action:
- because the co-analgesic drug must accumulate before it provides pain relief, and/or
- because therapy is initiated at low doses to avoid side effects.
Instant Feedback:
When using a coanalgesic with an opioid, the coanalgesic drug should be introduced first.
For patients with chronic nonmalignant pain, who are not medically ill, a co-analgesic may be the only drug taken by the patient on a regular basis. In the palliative care setting, co-analgesics are often given to patients who receive multiple drugs. Although this strategy is accepted practice for terminally ill patients, the potential for additive side effects and unpredictable adverse effects must be anticipated whenever a coanalgesic is added to an existing drug regimen.
Coanalgesic are used to enhance pain relief without serious risk or side effects. Additional pain relief at the expense of sedation or mental clouding is not acceptable for patients whose goals include restoration of function, but may be very appropriate for individuals who have pain relief as their only goal.
Antidepressant drugs – this group of drugs may be used as coanalgesics for many types of chronic pain syndromes. Antidepressant drugs enhance pain modulation by interfering with the re-uptake of serotonin and norepinephrine to decrease the perception of pain. Antidepressant drugs are started at a low dose. If the patient does not benefit from the usual analgesic dose and has no side effects, the dose may be titrated upward until the antidepressant dose is reached. A favorable analgesic effect is usually observed within a week. In some patients, maximal effect appears to evolve over several days or weeks. This delay, combined with the many days needed to increase the dose to a therapeutic level, may result in a prolonged period during which patients experience troublesome side effects and little positive pain relief benefit. Unless the patient is well informed about this potential, he or she is likely to discontinue the drug. Drug concentrations may be monitored during therapy.
Instant Feedback:
It may take some time for an antidepressant coanalgesic to reach a therapeutic effect.
Tricyclic antidepressants and selective serotonin re-uptake inhibitors (SSRIs) may be used to treat chronic neuropathic pain.
Examples of tricyclic antidepressants include:
- Amitriptyline (Elavil)
- Doxepin (Sinequan)
- Imipramine (Tofranil)
- Nortriptyline (Pamelor, Aventyl)
Examples of SSRIs include:
- Citalopram hydrobromide (Celexa)
- Fluvoxamine maleate (Luvox)
- Paroxetine hydrochloride (Paxil)
- Sertraline hydrochloride (Zoloft)
There are a number of side effects associated with antidepressants. Tricyclic antidepressants can cause orthostatic hypotension. This side effect is common in elderly individuals and, combined with the sedating effects of these drugs, place the patient at an increased risk for falls. Tricyclic antidepressants may also cause mental clouding, confusion, and somnolence. These drugs also produce hypotensive effects, such as dry mouth, blurred vision, and constipation. The most serious side effect of the tricyclic antidepressants, cardiotoxicity, is uncommon. Patients at increased risk of this complication include those who have significant heart disease, including conduction disorders and heart failure. Both tricyclic antidepressants and SSRIs can produce sexual dysfunction. Because of the side effects associated with tricyclic antidepressants, these drugs are usually used at low doses in addition to regular doses of SSRIs for concurrent depression.
Instant Feedback:
Elderly patients may be at increased fall risk when taking tricyclic antidepressants.
Anticonvulsants - Anticonvulsant drugs help control the ectopic, spontaneous firing of neurons in the central nervous system that produce seizures. It is thought that anticonvulsant drugs may also decrease the spontaneous firing of neurons in the peripheral nervous system that are associated with neuropathic pain.
Examples of anticonvulsant drugs include:
- Carbamazepine (Tegretol)
- Oxcarbazepine (Trileptal)
- Topiramate (Topamax)
- Valproic acid (Depacon)
- Tiagabine (Gabitril)
- Levetiracetam (Keppra)
- Phenytoin (Dilantin)
- Lamotrigine (Lamictal)
- Zonisimade (Zonegran)
- Gabapentin (Neurontin)
Corticosteroids - Corticosteroid drugs (Prednisone and others) may be used as coanalgesics in a variety of chronic pain syndromes (Yasir 2023). Their anti-inflammatory and analgesic effects are attributed to several mechanisms including:
- Corticosteroids reduce pain by reducing inflammation and edema associated with chronic inflammation, autoimmunity, tumours and depolarization of damaged nerves.
- Corticosteroids promote the synthesis of lipocortin-A (Annexin A1), a protein that:
- inhibits phospholipase A2 (Yasir, M. 2023). Inhibition of the Phospholipase A and its release of pro-inflammatory fatty acids (arachadonic acid) from the cellular membrane,
- limits neutrophil recruitment and production of their proinflammatory mediators (Sugimoto 2016)
- inducines neutrophil apoptosis, modulates monocyte recruitment, and enhances the clearance of apoptotic cells by macrophages(Sugimoto 2016)
- methylprednisolone has been shown to suppress the transmission in thin unmyelinated C-fibres while not affecting myelinated Aβ fibres and it is thought that this effect is via a direct membrane—stabilizing effect (Le DT, Alem N. 2023)
Corticosteroids are usually taken on a short-term basis and tapered off gradually. Serious adverse effects from systemic corticosteroids/glucocorticoid use increase with, dose, duration of therapy, and other factors associated with the patient’s medical condition. Potential adverse events from long-term use include:
- Musculoskeletal glucocorticoid induced osteoporosis, myopathy, osteonecrosis
- Metabolic and Endocrine adverse effects include:
- Diabetic and glucose intolerant patients exhibit higher blood glucose levels while taking glucocorticoids,
- Cushingoid fat redistribution and weight gain are dose and duration dependent,
- Hypothalamic-pituitary-adrenal (HPA) axis supression leading to adrenal atrophy symptoms
- weakness/fatigue, malaise, nausea, vomiting, diarrhea, abdominal pain, headache usually in the morning,
- fever, anorexia/weight loss, myalgia, arthralgia, psychiatric symptoms, poor growth and weight gain in children
- Immune supression leading to serious life threatening risk from common infectious agents.
- Neuropsychological effects can range from:
- mild euphoria or anxiety, with hypomanic or activated states are more common early in treatment and depression more common in longterm therapy. Psychosis is more common with doses above 20 mg per day.
- Sleep disturbances
- Akathisia (motor restlessness) is common.
- Persistant neuropsychological symptom are uncommon after discontinuation of therapy.
- Cardiovascular adverse effects, especially with the mineralocorticoids cortisol and cortisone can lead to fluid retention, edema, weight gain, hypertension, and arrhythmias by increasing renal excretion of potassium, calcium, and phosphate.
- Ophthalmologic Adverse Effects
- Cataracts, bilateral and slow progressing are more common at doses above 10 mg per day.
- Glaucoma may occur in patients receiving intraocular and high dose corticosteroids
- Central serous chorioretinopathy, the collection of subretinal fluid in the macular region seperates the retina from the photoreceptors, is a very rare adverse effect of either topical or systemic corticosterioid therapy
- Gastrointestinal (GI) adverse Effects include: gastritis, gastric ulcer formation, GI bleeding, pancreatitis, visceral perforation, and hepatic steatosis. Concomitant use of NSAIDS increases the risk of adverse effects 4-fold.
- Dermatologic adverse effects can occur even with low dose use of corticosteroids. These effects can include ecchymosis, skin thinning and atrophy, acne, mild hirsutism, facial erythema, stria, impaired wound healing, thinning of hair, and perioral dermatitis.
References
Imani, F., & Varrassi, G. (2019). Ketamine as Adjuvant for Acute Pain Management. Anesthesiology and pain medicine, 9(6). https://doi.org/10.5812/aapm.100178
Le DT, Alem N. Facet Joint Injection. [Updated 2023 Jun 20]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK572125/
Nwosu, A. D.George; Chukwu, L.C.; Onwuasoigwe, O; Nweze, S; Nwadike, K; Redefining the Role of Analgesic Adjuvants in Pain Management: A Narrative Review. Indian Journal of Pain 37(2):p 65-73.
DOI: 10.4103/ijpn.ijpn_23_22
Portenoy R. K. (2020). A Practical Approach to Using Adjuvant Analgesics in Older Adults. Journal of the American Geriatrics Society, 68(4), 691–698. https://doi.org/10.1111/jgs.16340
Sugimoto, M. A., Vago, J. P., Teixeira, M. M., & Sousa, L. P. (2016). Annexin A1 and the resolution of inflammation: Modulation of neutrophil recruitment, apoptosis, and clearance. Journal of Immunology Research, 2016, 1–13. https://doi.org/10.1155/2016/8239258
Yasir, M., Goyal, A., & Sonthalia, S. (2023). Corticosteroid Adverse Effects. In StatPearls. StatPearls Publishing
© RnCeus.com